Total Hip Replacement
Total hip replacement is considered when hip arthritis or another serious hip condition causes pain and mobility limits that are no longer adequately controlled with simpler treatments.
What the operation replaces
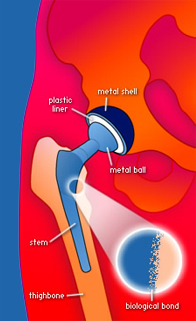
During total hip replacement, the damaged femoral head and the worn socket surface are removed. They are replaced with an artificial socket, liner, ball, and stem. The goal is to reduce pain, improve walking, and restore a smoother moving hip joint.
Implant fixation
Hip implants can be fixed to bone with or without bone cement. In an uncemented hip replacement, the implant is initially held by a tight fit and later by bone growing onto or into the porous surface. In a cemented hip replacement, surgical bone cement fixes the implant immediately. In my practice, I usually use uncemented total hip implants, while still individualizing the choice to the patient's age, bone quality, anatomy, and surgical situation.
More detail
The pages in this section explain who may benefit from surgery, what the risks are, the type of prosthesis used, the steps before surgery, surgical approaches, hospital stay, expected recovery, and revision surgery.
Frequently Asked Questions
When should hip replacement be considered?
Hip replacement may be considered when hip arthritis or another serious hip condition causes substantial pain and limitation despite reasonable non-surgical treatment. The decision should be based on pain, function, imaging, medical fitness, and how much the hip interferes with activities of daily living.
Do I need to bring x-rays or MRI images?
Yes. The radiology report alone is not enough. Please bring access to the actual images, usually through an online image access code or portal instructions. Some clinics still provide images on CD or DVD.
How long should I wait after a cortisone injection before hip replacement?
If a corticosteroid, or cortisone, injection was placed into the hip that is going to be replaced, elective hip replacement is generally delayed at least 3 months from the injection date. The strongest evidence of increased periprosthetic joint infection risk is when hip replacement is performed within 3 months after an injection into the same joint.
Please tell us the exact date, joint injected, and medication used. If hip replacement is likely soon, do not have another steroid injection into that hip without discussing timing. See the Injection Therapy safety page and this hip replacement infection-risk study.
How long will I stay in hospital?
About half of patients go home the same day after hip replacement. Others stay overnight, most often because of medical conditions, monitoring needs, pain control, dizziness, nausea, late surgery time, or home support concerns.
How long does recovery take?
Walking usually starts shortly after surgery. Many patients notice steady progress in the first few weeks, but overall rehabilitation commonly takes 3 to 4 months, with some improvement continuing longer.
When can I drive after hip replacement?
Most patients should not drive until they are off narcotic pain medication, can get in and out of the car safely, have enough strength and reflexes to control the vehicle, and can perform an emergency stop.
Scientific reviews and modern braking studies suggest that driving recovery after hip replacement is often in the 2 to 6 week range; about 6 weeks remains a conservative general guideline. The timing should be individualized based on the side of surgery, vehicle type, medication use, confidence, and overall recovery.
Do I need antibiotics before dental procedures after hip replacement?
For most patients with a hip replacement, routine antibiotics before dental procedures are not recommended solely to protect the artificial joint. The Canadian consensus statement from the Canadian Orthopaedic Association, Canadian Dental Association, and AMMI Canada, the American Dental Association guideline, and the 2024 AAOS/AAHKS guideline do not support routine antibiotic prophylaxis for most patients.
Good oral hygiene and prompt treatment of dental infection are important. Patients with previous joint infection, major complications, significant immune suppression, poorly controlled diabetes, or other special risk factors should discuss their situation with their dentist and surgeon before invasive dental work. Some patients may need antibiotics for other medical reasons, such as certain heart conditions, which should be decided by the dentist or physician managing that condition.
Does the surgical approach determine the long-term result?
No single approach has been proven to give better long-term results for every patient. I use a modified direct superior approach, which is muscle splitting, and I individualize decisions based on anatomy, safety, and reliable implant positioning.
Can I return to sports after hip replacement?
Most patients are encouraged to return to regular physical activity after recovery. Low-impact sports such as walking, cycling, swimming, golf, hiking, and gym-based conditioning are usually the safest choices.
Intermediate-impact activities usually involve more force, uneven ground, or some twisting, such as doubles tennis, pickleball, skating, cross-country skiing, downhill skiing on groomed runs, or more demanding hiking. High-impact activities include running, jumping sports, singles tennis, basketball, soccer, hockey, football, rugby, squash, racquetball, martial arts, and high-impact aerobics.
A recent review of return to sport after hip and knee arthroplasty recommends low-impact sports, allows many intermediate-impact sports when the patient has previous experience, and generally discourages high-impact sports unless discussed individually. A hip replacement umbrella review reached similar conclusions. Timing should be gradual and individualized; many patients begin lower-impact activity around 3 to 6 months, while a fuller return to recreational sports often takes closer to 6 to 12 months.